COVID-19 Emergency Situation Report 19 (22 September – 5 October 2020)
Highlights
- Over 6,000 new COVID-19 cases recorded in the OPT, but active cases decline significantly; 88 more people die.
- 1,000 more cases of community transmission, and another six fatalities reported in Gaza.
- The general lockdown is extended in both the West Bank and Israel, which also includes annexed East Jerusalem.
- The Inter-Agency Response Plan for the OPT is 47 per cent funded.
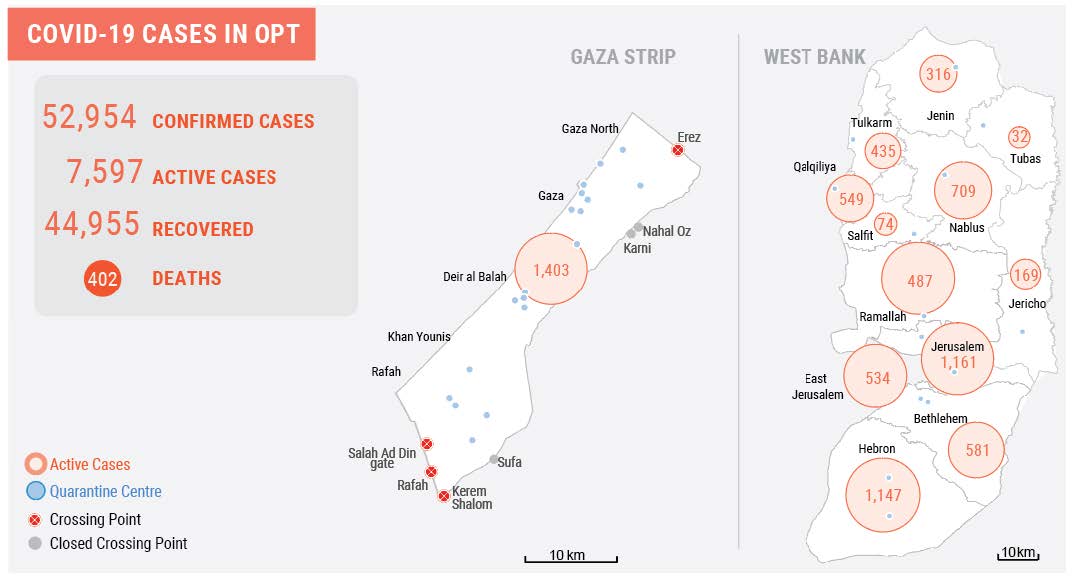
| 7,597 | 52,954 | 402 | US$72.2 M |
| Active COVID-19 cases | Cumulative Total COVID-19 Cases | Fatalities | Request for Inter-Agency Response Plan |
Situation Overview
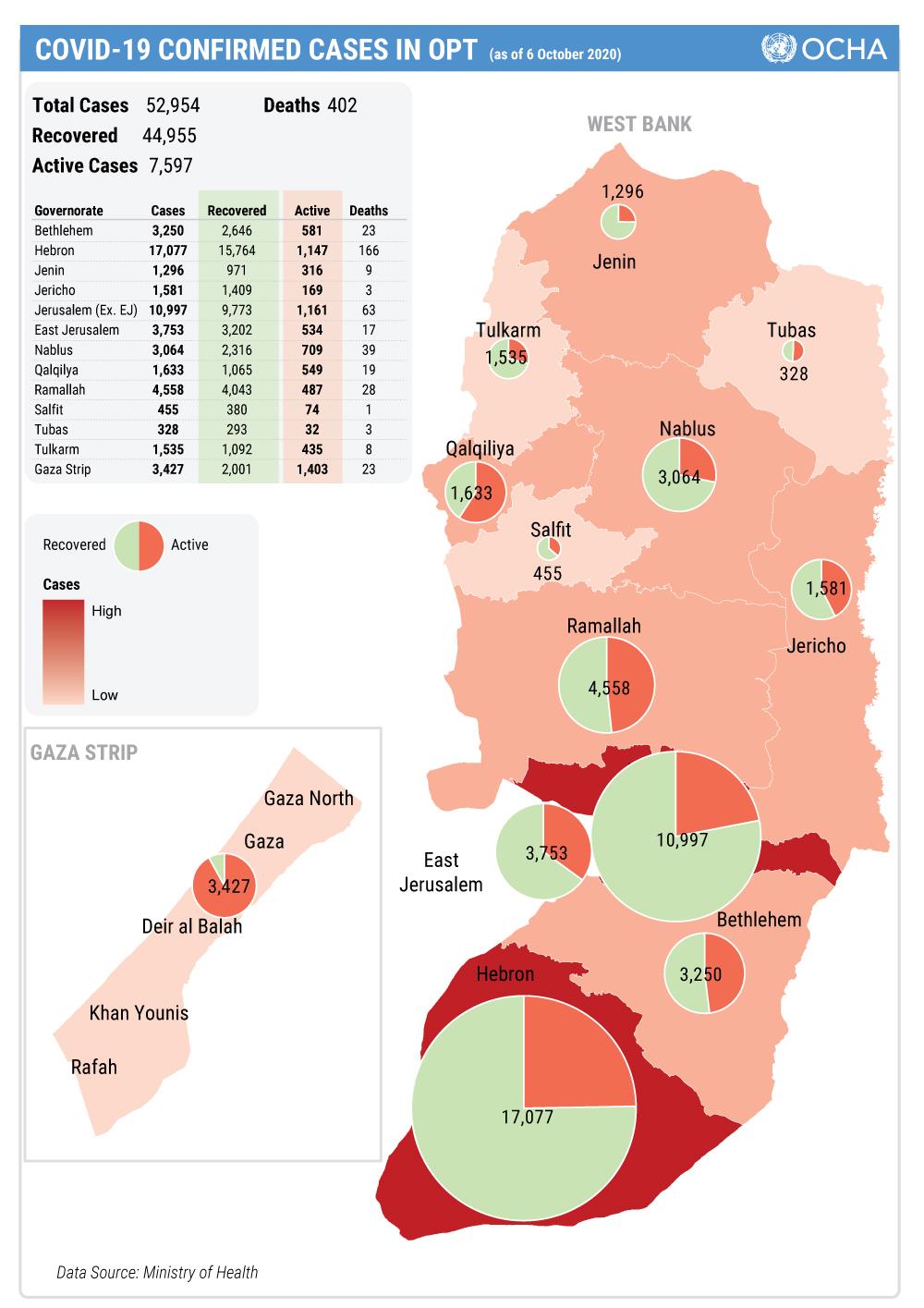
During the reporting period, some 6,350 additional Palestinians in the OPT tested positive for COVID-19, bringing the cumulative number of cases since the start of the crisis to approximately 53,000 (as of 16:00, 5 October). Eighty-eight more people died, bringing to 402 the cumulative number of fatalities due to the virus, 379 in the West Bank, including East Jerusalem, and 23 in the Gaza Strip. Forty-seven patients are in intensive care units (ICU), eleven of whom require mechanical ventilation, according to the Ministry of Health (MoH).
More than 11,000 people recovered during this period, and the number of active cases decreased by 40 per cent, from 12,698 to 7,597. However, due to the shortage of testing kits in the West Bank, only Palestinians who are traveling and those exhibiting symptoms of COVID-19 can be tested. Others are asked to self-isolate for 14 days.
Some 85 per cent of patients have now recovered from the virus and the case fatality rate remains low at 0.8 per cent. Hebron and East Jerusalem account for over 50 per cent of cumulative cases, although Gaza now has the largest share of active cases (18 per cent). The positivity rate for those tested in the West Bank is around 14 per cent. In Gaza, the number of tests conducted per day is around 2,000, with a positivity rate between three and five per cent. The ability of the Gaza healthcare system to manage the surge in COVID-19 cases continues to be of significant concern.
On 2 October, in the West Bank, the Palestinian Authority (PA) declared an extension of the state of emergency for 30 days. In Israel, the general lockdown, applicable also to annexed East Jerusalem, which started on 18 September, has been extended to 14 October. In Gaza, lockdown measures imposed since August remain, although the authorities have eased some of the restrictions.
West Bank
The number of cases who display serious COVID-19 complications is increasing in Bethlehem and Hebron, leading to a higher demand for ICU beds. Due to an increase in the number of confirmed cases, the Jenin and Tulkarm governorates were placed under a three-day closure on 3 and 4 October respectively, closing down institutions and public places, and minimizing movement. A number of schools are partially shut down for 24 to 72 hours in Tulkarm and Salfit.
All wedding halls and mourning houses remain closed. There has been an increase in the enforcement of COVID-19 restrictions in all governorates, resulting in fines for violations by individuals and businesses, except in Area C and the Israeli-controlled area of Hebron city (H2), where the Palestinian police has no jurisdiction. Enforcement of restrictions by Israeli police in East Jerusalem has also increased.
All active cases that do not require medical treatment are being referred to home quarantine. In preparation for a continuing surge in infection, 13 facilities across the West Bank have been placed on stand-by to receive people who test positive but do not have suitable conditions for home isolation; ten of these isolation centres are supported by UNRWA to serve residents of refugee camps, primarily. In East Jerusalem, an isolation centre has already been activated at the Seven Arches Hotel and is hosting 22 people. Most hospitals across the West Bank, including in East Jerusalem, have opened dedicated wards to treat people suffering from more serious symptoms.
With the support of the Education Cluster, all schools in the OPT have received cleaning and hygiene kits, copies of the Safe Schools and Health protocols and related training. Since 20 September, schools have reopened in the West Bank, although around 90 schools have either temporarily, or fully, closed for instances of between one and 14 days, following confirmed COVID-19 cases among pupils or school staff. On 23 September, a strike by teachers and staff started in certain West Bank schools to protest the PA’s non-payment of salaries.
Despite the lockdown in Israel, Palestinian workers in the construction, agricultural and health sectors continue to cross checkpoints to their jobs in Israel, upon displaying valid permits. Workers in other sectors are denied entry. Increased efforts are reported on the part of Israel security forces to prevent the smuggling of workers through informal openings in the Barrier, including through the use of force: since the outbreak of the pandemic, Israeli forces have injured at least 66 Palestinians in this context, including 23 by live ammunition.
Between 19 September and 4 October, 1,684 Palestinians entered the West Bank through the Allenby Crossing with Jordan, and 2,014 departed. All such movements require prior coordination with the Palestinian Ministry of Foreign Affairs and testing for COVID-19 before crossing in either direction.
Citing the lack of building permits, during the reporting period, the Israeli authorities demolished or seized 42 Palestinian-owned structures in Area C and East Jerusalem, displacing 53 people and affecting the livelihoods or access to services of over 150 others. Since the start of the pandemic, the Israeli authorities have demolished or seized, or forced people to demolish, at least 460 structures; this represents a 60 per cent increase compared with the monthly average between 2017 and 2019 (66 vs. 41).
On 1 October, in reply to a letter from the Civic Coalition for Palestinian Rights in Jerusalem and Adalah, an Israeli NGO, the Israeli Justice Ministry agreed to re-implement a policy introduced in March, in response to the first wave of the COVID-19 pandemic, to stop the demolition of inhabited residential buildings in East Jerusalem. The agreement does not apply to structures built after 1 October. The issuance of administrative demolition orders will be reduced in general, so that orders are only issued in relation to new construction, particularly that which is judged to take advantage of the state of emergency.
Gaza Strip
In Gaza, approximately 1,000 new COVID-19 cases were recorded in the reporting period. The number of active cases declined from 1,780 to 1,403, out of a total of 3,427 cases overall. Six fatalities were recorded, bringing the total number to 23. Gaza City and Northern Gaza continue to account for about 85 per cent of active cases, almost all of which are attributable to transmission within the community.
Confirmed cases displaying symptoms are being isolated in the European Hospital and the Turkish Hospital. People who have no or light symptoms, who constitute the vast majority of active cases, are sent to home isolation, or to one of two designated facilities in Khan Younis and Deir al-Balah.
The lockdown measures imposed since late August remain, although the authorities have eased some of the restrictions. Movement between governorates has resumed, and mosques, shops, supermarkets, barbershops and other facilities in the less affected ‘green’ and ‘yellow’ zones have been allowed to reopen. Adherence to health measure in these facilities, as well as on the streets, is still being enforced by the local police who maintain a heavy profile. Essential government staff have also resumed working from offices. A lockdown remains in place only in parts of Gaza city and all of Northern Gaza.
On 4 October, mosques reopened in the governorates of Rafah, Khan Younis and the Middle Area. Measures such as social distancing and mandatory wearing of masks continue to be applied, and mosque workers are obliged to clean and disinfect the mosques daily and ensure good ventilation. Mosques in the governorates of Gaza City and North Gaza, as well as in one neighbourhood of Khan Younis where a cluster of cases was detected, remain closed. The MoEHE is planning to gradually reopen schools, as of 10 October, starting with students in grade 12, Tawjihi.
Between 27 and 29 September, for the first time since 13 August, the Rafah Crossing with Egypt opened for three days. During that period, 1,700 Palestinians entered Gaza, and 2,659 exited. Those entering were immediately directed to quarantine and isolation facilities: quarantine in such facilities has being further reduced from 14 to seven days, with people self-quarantining at home for an additional seven days.
Over 1,900 people, including returnees and isolated suspected cases, are currently in these facilities across Gaza, which include hotels, schools, hospitals and health centres. The majority of people in quarantine will be discharged this week, as the authorities conduct tests and release those with negative results. Over 9,000 individuals (approximately 1,700 families) are reported to be in home quarantine/isolation, more than 60 per cent of these in Gaza City.
The Qatar Committee for the Reconstruction of Gaza, the main food provider for those in the quarantine facilities, announced that, as of 6 October, it will stop the provision of food to these facilities, due to the lack of dedicated funds to continue this support.
The entry of goods continued from Israel through the Kerem Shalom Crossing, as did imports from Egypt via the Rafah Crossing. The Erez passenger crossing with Israel was also open for the movement of a small number of exceptional cases (mostly patients). The Rafah passenger crossing has closed again, following the exceptional three-day opening, mentioned above.
Coordination
The Inter-Agency COVID-19 Task Force, led by the Resident/Humanitarian Coordinator (RC/HC), as well as the Inter-Cluster Coordination Group (ICCG), continues to convene on a weekly basis, to set policies and coordinate the implementation of various responses to the crisis.
Since the imposition of the Gaza lockdown on 24 August, the RC/HC’s Access and Coordination Unit (ACU) has been coordinating the movement of humanitarian staff within Gaza with the local authorities, to facilitate critical missions. Interested organizations submit their requests for coordination through an online system. These are reviewed by the relevant cluster lead, the ICCG Chair and the ACU, and submitted to the authorities. Through its 24/7 hotline, the ACU assists in solving problems faced by staff on approved missions. So far, the ACU has facilitated 474 critical missions.
Since 6 September, the World Health Organization (WHO) has been operating a temporary coordination mechanism to support Palestinian patients and companions from Gaza to apply for Israeli exit permits to access essential health services in hospitals in the West Bank and Israel. Referrals are made according to medical need, as decided by the Palestinian MoH. This temporary measure has been taken to mitigate the impact of the PA halt of coordination with the Israeli authorities, adopted since May, in response to Israel’s threat to annex part of the West Bank.
In the same context, the UN Country Team has continued to operate a Logistics Cluster, led by the World Food Programme (WFP), to support the procurement of supplies and the receipt of donations needed for the COVID-19 response. Its main task is to mediate between the Customs Directorate in the PA Ministry of Finance and the Israeli authorities (COGAT and the Israeli Customs Office) to ensure the approval of the documentation required to allow the shipment of imported supplies into the OPT, through the various Israeli ports of entry. The cluster has processed 92 requests from UN agencies and international NGOs, of which 74 have been approved by both sides, 13 are pending approval by the Israeli authorities, and five were cancelled.
The Health Cluster is tracking the procurement and delivery of critical medical supplies by cluster partners against the immediate needs identified in the COVID-19 Inter-Agency Response Plan, in line with the State of Palestine’s National Response Plan. The following table highlights the availability and gaps regarding the top ten medical items needed.
[1]
All partners are encouraged to subscribe and submit their requests for procurement of medical supplies for laboratory testing, case management and infection prevention and control through WHO’s global COVID-19 response coordination portal.
As part of the Risk Communication and Community Engagement (RCCE) plan, nearly 40 partners are distributing communication materials aimed at ensuring that the public has access to a broad range of information on how to prevent the spread of COVID-19, and to deal with misinformation, as restrictions are eased, or alternatively re-imposed, by the respective authorities. To address the sudden escalation in cases in Gaza, the campaign has broadcast radio messages daily on six channels in Gaza; and released an Emergency Media Pack with social media materials, videos, brochures and radio resources to media and NGOs in Gaza, among other measures. RCCE materials are available online.
| Supply Category | Medical item | Estimated Response Plan needs (by unit) |
Delivered | Pipeline/procured | Current Gap |
| Case Management | Ventilator, medical, invasive, adult/child | 250 | 54 | 166 | 30 |
| Patient Monitor (vital signs) | 250 | 40 | 189 | 21 | |
| Oxygen Concentrator | 250 | 15 | 159 | 76 | |
| ICU Hospital Beds | 250 | - | 166 | 84 | |
| Patient Beds | 400 | 86 | 264 | 50 | |
| Infection Prevention and Control (IPC) | Surgical Mask | 4,000,000 | 1,460,150 | 216,550 | 2,323,300 |
| N-95 Respirator | 300,000 | 62,748 | 168,380 | 68,872 | |
| Surgical gloves | 8,000,000 | 3,984,000 | 1,633,800 | 2,382,200 | |
| Laboratory Testing | COVID-19 PCR Tests | 500,000 | 83,712 | 9,600 | 406,688 |
| Swabs / Medium, sample collection | 500,000 | 44,500 | 455,500 |
Funding
The initial COVID-19 Inter-Agency Response Plan for the OPT, which requested $42.4 million to support an immediate response to the crisis and the efforts led by the Government of Palestine, covered interventions through the end of June. In August, the Plan was extended until the end of 2020 and the financial requirement updated to $ 72 million.
During the reporting period, an additional contribution of $274,983 was received from the UK Foreign, Commonwealth and Development Office (FCDO) for the Health Cluster. This brings to $33.8 million the funding raised since the start of the crisis, or 47 per cent of the amount requested in the Response Plan. Including resources contributed outside the Response Plan, a total of $52.8 million have been mobilized in support of COVID-19 related response activities in the OPT.
So far, the overall response to COVID-19 has been generously supported by donors. The recent escalation of the pandemic requires sustained efforts to continue responding to the full scale of needs of vulnerable people across the OPT.
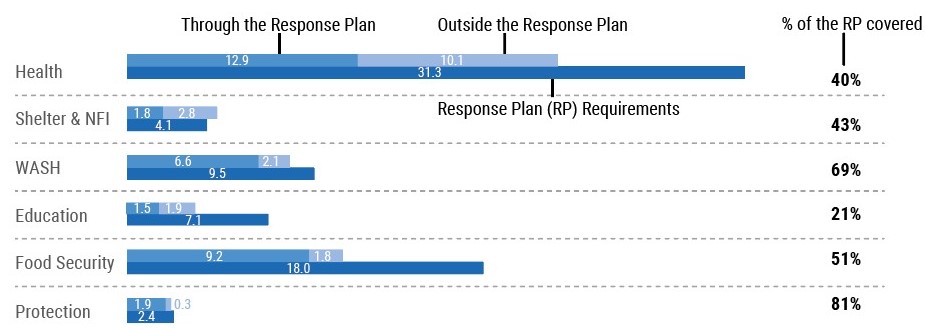
Total funding for COVID-19 response by cluster (in Million US$)
Developments, concerns and funding status by cluster
Health
| US$31,304,992 | $12,905,035 | 41% | US$ 10,125,602 | US$ 23,030,637 |
| Funding requirements | Through the Response Plan | of the RP covered | Outside Response plan | Total Funding Received |
- The number of confirmed COVID-19 cases continue to rise, while the case fatality rate remains low at 0.8 per cent. More than two-thirds of all the newly reported cases in the West Bank are in the Hebron and Jerusalem governorates.
- In Gaza, contagion within the community remains of serious concerns due to capacity gaps in the health system. Health Cluster partners continue to address key priorities, including to scale-up testing and contact tracing; case management capacity; and risk communication and community engagement. The protection of frontline health workers continues to be prioritized by ensuring adequate quantities of personal protective equipment (PPE) and the dissemination of knowledge and skills in infection prevention and control (IPC). As of 4 October, 96 health workers across Gaza have been infected with COVID-19.
- Nearly 155,000 people have benefited from activities carried out by Health Cluster partners during the reporting period. Across the OPT, partners delivered 20,000 swabs and laboratory supplies to conduct 84,000 COVID-19 tests, in addition to essential medical equipment to the Ministry of Health in Ramallah, including portable ECGs; patient monitors; oxygen flowmeters; intravenous poles; face shields; ventilators; hospital beds and mattresses; and surgery tables.
- An assessment of the European Gaza Hospital was conducted to evaluate the ICU, as well as to review the protocols, IPC, nursing care and patients flow. In addition to the COVID-19 related response, partners are also working to support other essential healthcare services, including mental health and psychosocial support (MHPSS) and support to patients with non-communicable diseases.
Protection
| US$ 2,365,740 | US$ 1,917,434 | 81% | US$ 305,434 | US$ 2,222,868 |
| Funding requirements | Through the Response Plan | of the RP covered | Outside Response plan | Total Funding Received |
- During the reporting period, Protection Cluster partners provided remote and in-person psychosocial support (PSS) to over 2,300 vulnerable people across the OPT. Another 61 children in the West Bank and Gaza received support with specialized case management, while awareness raising messages related to COVID-19 and Child Protection and Psychosocial Support Principles were disseminated to over 6,100 people.
- During the reporting period, one Gender-Based Violence (GBV) Sub-Cluster partner provided 50 per cent more phone consultations than in the previous period. However, partners continue to face challenges, including due to ongoing power cuts in the Gaza Strip; a need to protect field staff from contracting COVID-19 during service provision; a lack of capacity building opportunities for GBV staff on providing remote service counselling; and the inaccessibility to phones or privacy for GBV survivors to access GBV services.
Education
| US$ 7,120,698 | US$ 1,517,000 | 21% | US$ 1,918,746 | US$ 3,435,746 |
| Funding requirements | Through the Response Plan | of the RP covered | Outside Response plan | Total Funding Received |
- As of 20 September, all children have returned to schools across the West Bank. With the support of the Education Cluster, all schools in the OPT received cleaning and hygiene kits, copies of the Safe Schools and Health protocols and related training. Since the start of the school year, around 90 schools were either temporarily or fully closed from one to 14 days, following confirmed COVID-19 cases among pupils or school staff. The current situation is imposing additional challenges to ensuring the continuity of face-to-face education during the spread of the pandemic.
- All education facilities in the Gaza Strip remained closed since 24 August. The MoEHE is planning to gradually reopen schools, as of 10 October, starting with pupils in Grade 12. No dates are announced for the other grades.
- The Education Cluster is working with the Ministry of Education (MoE) and UNRWA to support the delivery of distance learning, MHPSS services, IPC measures and provision of hygiene kits and rehabilitation of WASH facilities.
Shelter & NFI
| US$ 4,092,551 | US$ 1,755,251 | 43% | US$ 2,767,382 | US$ 4,522,633 |
| Funding requirements | Through the Response Plan | of the RP covered | Outside Response plan | Total Funding Received |
- During the reporting period, Shelter Cluster partners provided Non-Food items (NFIs) to all active quarantine facilities in the Gaza Strip. As part of the response to people returning through the Rafah crossing, partners distributed over 3,600 NFI kits, including nearly 2,300 bedding items and 760 individual hygiene kits to people in quarantine and isolation centres in the Gaza Strip. Another 600 hygiene kits were distributed to households lacking proper hygiene facilities in home quarantine.
Water, Sanitation and Hygiene
| US$ 9,504,052 | US$ 6,571,005 | 69% | US$ 2,081,548 | US$ 8,652,533 |
| Funding requirements | Through the Response Plan | of the RP covered | Outside Response plan | Total Funding Received |
- The WASH Cluster reached around 3,700 people during the reporting period. In the Gaza Strip, three partners delivered nearly 58,000 bottles of water and 830 dignity kits to people in 13 quarantine centres, in addition to the emptying of septic tanks of more than 100 households. Fifty households in Area C of the West Bank and the H2 area of Hebron received hygiene kits and WASH items.
- The WASH cluster is mapping its partners’ capacities to provide the WASH needs of people in quarantine, both in centres and at home, in Gaza, until the end of 2020. The responses to be covered include drinking water, garbage collection and hygiene materials.
- The WASH Cluster and the Ministry of Social Development (MoSD) have expanded the eligibility criteria for WASH assistance to households with a family member in home quarantine. The most vulnerable families in the OPT with confirmed COVID-19 cases will receive hygiene and disinfection materials to support necessary protection measures to mitigate the spread of the virus.
Food Security
| US$ 18,017,577 | US$ 9,177,426 | 51% | US$ 1,777,441 | US$ 10,954,867 |
| Funding requirements | Through the Response Plan | of the RP covered | Outside Response plan | Total Funding Received |
- As emergency food distribution is crippled by COVID-19 restrictions, households across the OPT are struggling to meet their basic food needs. The nutritional status of new vulnerable groups in the Gaza Strip is deteriorating, while farmers are facing decreased harvest quantity and quality due to the lockdown.
- Agriculture and livelihoods continue to be severely affected in the Gaza Strip: while traders had inputs in stock, these remained partially inaccessible due to movement restrictions. Farmers and breeders are buying on credit, and traders suffer from insufficient financial liquidity, placing them at risk of losing their ability to import agricultural inputs.
- Food shortages are expected in quarantine and isolation centres in Gaza, following a halt in the funding provided to such centres by the Government of Qatar.
- The Food Security Cluster is working with the Ministry of Social Development (MoSD) in Gaza to identify additional need among those most affected by the lockdown. Additional food assistance to the most vulnerable families, as well as cash support, is urgently needed.
COVID-19 response funding in the OPT (through and outside the Inter-Agency Response Plan) in US$
| Cluster | Response Plan Requirements (US$) | Through the Response Plan (US$) | Percentage of the Plan covered | Outside the Response Plan (US$) | Total (US$) |
| Education | 7,120,698 | 1,517,000 | 21% | 1,918,746 | 3,435,746 |
| Food Security | 18,017,577 | 9,177,426 | 51% | 1,777,441 | 10,954,867 |
| Health | 31,304,992 | 12,905,035 | 41% | 10,125,602 | 23,030,637 |
| Protection | 2,365,740 | 1,917,434 | 81% | 305,434 | 2,222,868 |
| Shelter & NFI | 4,092,551 | 1,755,251 | 43% | 2,767,382 | 4,522,633 |
| WASH | 9,504,052 | 6,571,005 | 69% | 2,081,548 | 8,652,553 |
| Total | 72,405,610 | 33,843,150 | 47% | 18,976,153 | 52,819,303 |
Total funding for COVID-19 response by donors
|
Donors |
Through the Response Plan |
Outside the Response Plan |
Total in US$ |
|
Austria |
|
229,564 |
229,564 |
|
Canada |
2,215,757 |
|
2,215,757 |
|
CERF |
527,000 |
|
527,000 |
|
DFID |
1,423,772 |
|
1,423,772 |
|
ECHO |
3,720,950 |
6,491,0001 |
10,211,950 |
|
Education Cannot Wait |
555,000 |
1,550,000 |
2,105,000 |
|
Foreign Disaster Assistance (OFDA) |
225,000 |
|
225,000 |
|
France |
1,005,415 |
|
1,005,415 |
|
Germany |
4,042,854 |
43,000 |
4,085,854 |
| Ireland (Irish Aid) | 235,200 |
|
235,200 |
|
Islamic Relief Worldwide |
307,800 |
|
307,800 |
|
Italian Agency for Development Cooperation [AICS] |
152,008 |
10,970 |
162,978 |
|
Japan |
878,506 |
|
878,506 |
|
Kuwait |
747,500 |
8,252,500 |
9,000,000 |
|
Norway |
70,000 |
91,083 |
161,083 |
|
OPT Humanitarian Fund2 |
6,734,970 | 347,768 | 7,082,738 |
|
Other sources3 |
1,461,198 |
330,155 | 1,791,353 |
|
Private Sector Fundraising |
386,786 |
|
386,786 |
|
Qatar Fund for Development |
|
562,455 |
562,455 |
|
Qatar Red Crescent |
|
410,000 |
410,000 |
|
Save the Children4 |
326,435 |
|
326,435 |
|
Start fund |
251,000 |
|
251,000 |
|
Sweden (SIDA) |
500,000 |
|
500,000 |
|
Swiss Agency for Development and Cooperation “SDC” |
1,450,000 |
268,000 |
1,718,000 |
|
UNFPA Humanitarian Thematic Fund |
332,000 |
|
332,000 |
|
UNICEF |
792,000 |
|
792,000 |
|
USAID |
250,000 |
|
250,000 |
|
War Child Holland5 |
252,000 |
85,000 |
337,000 |
|
WFP (loan) |
5,000,000 |
|
5,000,000 |
|
World Vision International |
|
304,658 |
304,658 |
|
Grand Total |
$33,843,150 | $18,976,153 | $52,819,303 |
|
1 Attribution to the Inter-Agency COVID-19 Response Plane under verification. 2 As of today, OPT Humanitarian Fund has received generous contributions from Germany ($13.8m), Belgium ($4.3m), Sweden ($2.1m) Switzerland ($2m), Norway ($0.9m), Iceland ($0.4m), Ireland ($0.3m), Korea ($0.3m), and Cyprus ($12,500). 3 Funding contributions below $150,000 including funding towards and outside Covid-19 Response Plan, received from: Action Aid, AECID, African Women Development Fund, AICS, Cantabria 19, Care International Emergency Fund, Christian Aid&ACPP, Denmark, DRO, EIHDR, Federal Ministry for Economic Cooperation and Development (BMZ), Fridresh Nauman Foundation, Gazze Destek (GDD), Global fund for women, Grass Roots, HEKS, Holland, ICO-UAE, International Charity Organisation, IR – Canada, IR – UK, Italy (IADC), Jerrahi Order of America, Kvinna Till Kvinna, Luxemburg government - ARDI Program, McNulty Foundation, Medico International, Mennonite Central Committee, Mixed funds (German, Italian, Spanish and Dutch), NCA, DCA, NMFA, Norwegian Representative Office to the Palestinian Authority, Nous Cims, NRC, Open Society Foundation, Oxfam, PHG, Private Donors, Rawa Funds, Representative Office of Switzerland in Ramallah, Secours Islamique France, SIDA+DFAT, StartNetwork, Suisse Cooperation, Trocare, UN Trust Fund, UNDP, United Palestinian Appeal, UNWOMEN HQ, Urgent Action Fund, WELFARE (Taawon), WHO, World Vision USA. 4 This includes contributions of Save the Children individual and pooled funds. 5 This includes contributions of War Child Holland and War Child Holland Head Office. |
|||
[1] For a more comprehensive list, please contact the Health Cluster Coordination Team: [email protected] and [email protected].
subscribe to our mailing list
SUBSCRIBE TO RECEIVE OCHA'S INFORMATION PRODUCTS
OCHA Sites








Follow Us
Support
Your donations go to relief organizations delivering quick and effective support to Palestinians in need.